


Calcific Tendinitis
Introduction
Calcific tendinitis is a condition where the body “over-reacts” and deposits calcium in the rotator cuff tendon. There are two (2) distinct variants of this problem; acute calcific tendinitis and chronic calcific tendinitis.
The treatment for each is slightly different, hence it is important to distinguish between the two. Before we look at this condition in greater detail, basic knowledge of the anatomy of the shoulder is necessary.
Anatomy of the Shoulder Joint
The shoulder joint is made up of 3 bones: the shoulder blade (scapula), the humeral head and the collar-bone (clavicle).
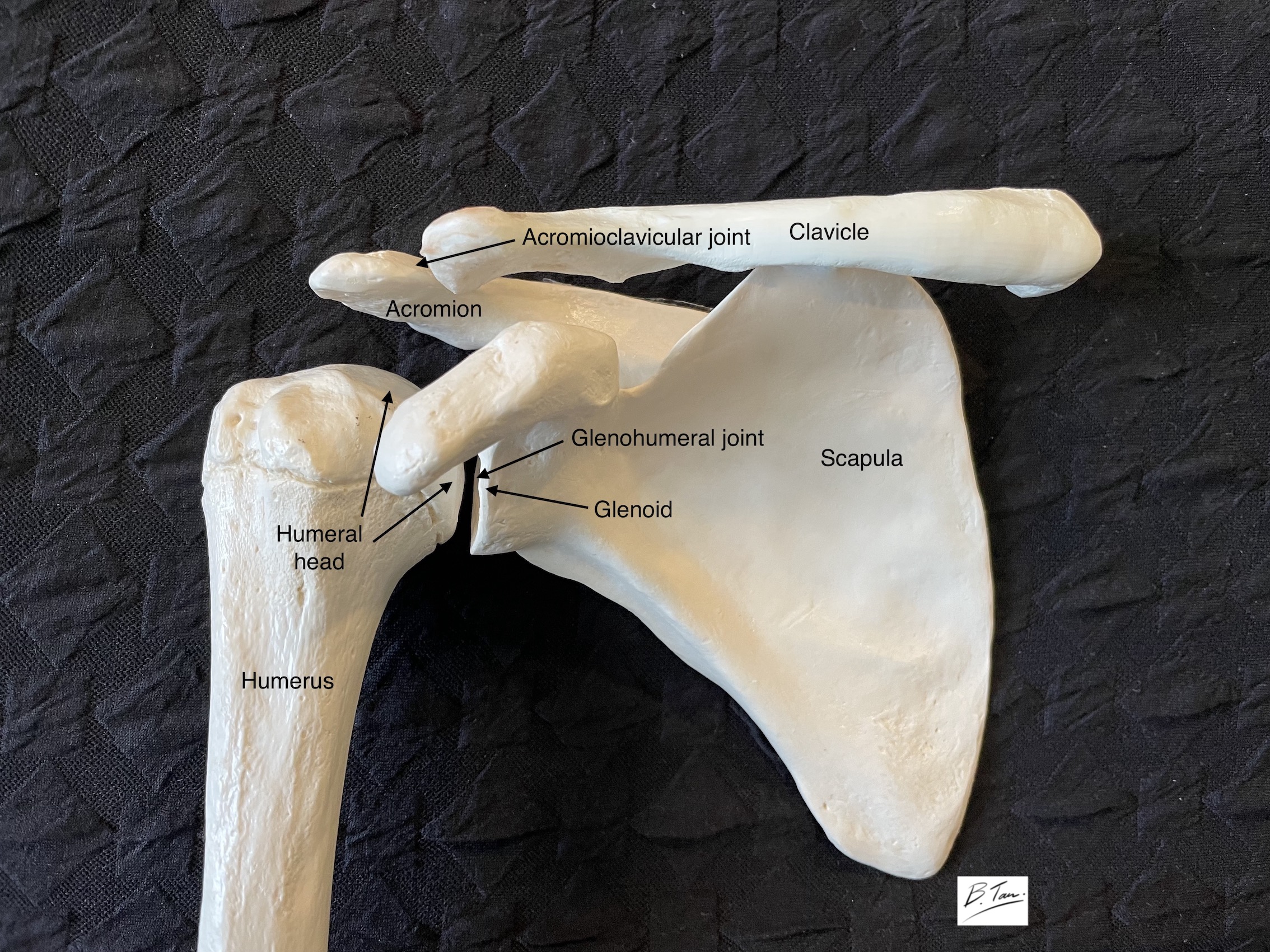
Movements around the shoulder involve 3 separate articulations: the glenohumeral joint, the acromioclavicular joint and the scapulothoracic articulation. When the arm is raised, the majority of movement occur at the glenohumeral joint and the scapulothoracic articulation.

Four (4) muscles are attached to the scapula and send their respective tendons across the glenohumeral joint and attach to the humerus just beyond the humeral head.
These 4 tendons are collectively known as the rotator cuff. You can think of the muscles as motors and their tendons as pulleys. Contractions of the muscles will hence bring about movement at the joint that their tendons cross.
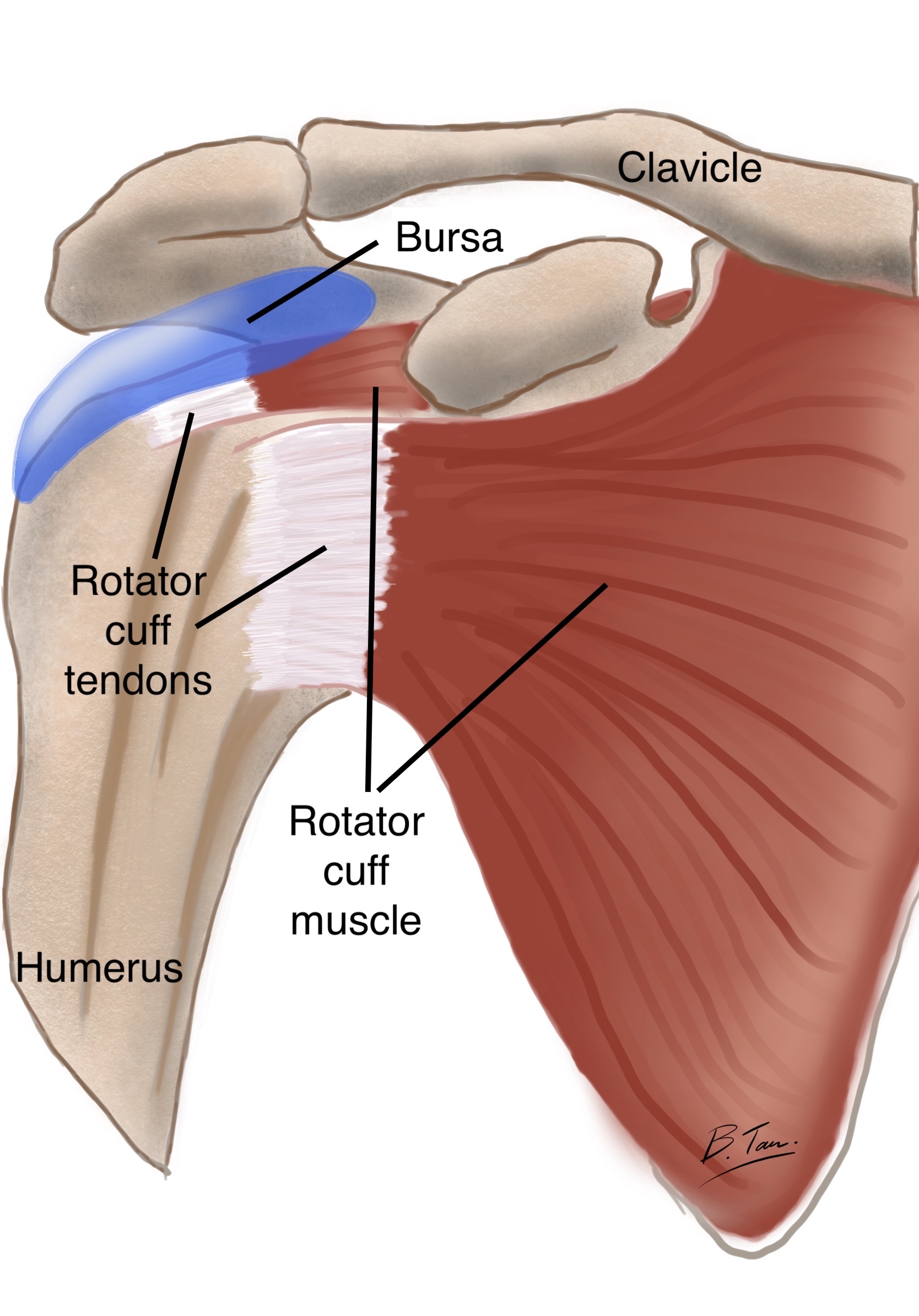
A part of the scapula, known as the acromion, forms a roof over the humeral head and rotator cuff (see picture of bony anatomy of the shoulder).
To reduce friction between the acromion and the underlying rotator cuff during shoulder movements, a thin sac containing a sliver of fluid sits on the superior surface of the rotator cuff. This sac is known as the bursa
What symptoms might I experience?
The main symptom that patients experience is pain. The pain that patients with acute calcific tendinitis feel is quite different from that of chronic calcific tendinitis.
Acute Calcific Tendinitis
The pain is usually very severe and comes on very quickly. Most patients will report that they were feeling absolutely normal, went to sleep then woke up in the next middle of the night or the next morning with such severe pain in their shoulder that they are unable to move it at all.
The pain is often severe enough with the arm held completely still, but any small movements are excruciating. Many patients come in hunched over, cradling their arms trying to minimize movements at the shoulder joint while they walk.
Chronic Calcific Tendinitis
The onset of pain is usually much more gradual. Many patients will report that they have been having discomfort and pain in their shoulders with certain movements. But because the pain is typically milder in nature, they had simply ignored it until either it gradually became worse, or the patients finally decided that they had put it off for too long and were seeking answers.
There is often little to no pain at rest, though some patients may have a mild background aching sensation. But movements, especially overhead movements, will cause pain. The pain is often not unbearable, but annoying enough to make patients avoid overhead movements.
As a result, they often develop stiffness as well. The stiffness is not severe but apparent when compared to the other unaffected side.
What will the doctor do?
Your doctor will chat with you and ask you more about your symptoms. A careful examination of the shoulder is then carried out. He (I will use “he” to refer to the doctor to simplify the discussion although clearly, there are many female doctors out there!) will need to visually inspect your shoulders, looking out for any asymmetry or wasting of the muscles.
He then feels around the shoulder looking for any tender spots which may give a clue as to the source of the problem. This may be particularly hard in large or muscular patients.
He then tests your shoulder movements and the strength in each of the rotator cuff muscles. Finally, he will usually carry out some clinical tests designed to elicit discomfort, in an effort to clinch the diagnosis.
Further imaging will usually be required to confirm his suspicions.
What tests can be done to confirm the diagnosis?
X-rays will usually reveal the problem. Often times, I will also order an MRI scan in order to assess the condition of the rotator cuff.
I generally shy away from ultrasound scans because it does not give me much additional information. In addition, the calcium deposit often casts a shadow (acoustic shadow) hence obscuring details about the tendon.
Please refer to the section on Investigations to learn more about the various forms of investigations.
What exactly, is calcific tendinitis?
Calcific tendinitis is a condition where calcium is deposited in or just on top of the rotator cuff tendon. The deposit is typically near the attachment of the tendon on the humerus. The calcium is deposited in the form of calcium hydroxyapatite crystals.
In acute calcific tendinitis, the calcium deposit is often the consistency of a paste. Much like toothpaste.
In chronic calcific tendinitis, the calcium deposit is often hard as a piece of chalk. However, it can be broken up easily with surgical instruments to be removed.

Why does the body deposit calcium like this?
Nobody knows why this condition occurs. Occasionally it can be associated with endocrine disorders like diabetes, but most of the patients that I have seen with calcific tendinitis have absolutely no systemic illnesses at all.
Who gets calcific tendinitis?
This condition almost never affects young patients, so I have never seen it occur in any patient under the age of 30. Most of the patients are in their 40s to 50s. It is also slightly more common in females than in males. Aside from age and gender, there seems to be little else that can help with predicting who may develop this problem.
Calcium is everywhere in the body! Bones are made of calcium. Why would calcific deposits cause pain?
Indeed, the exact cause of calcific tendinitis, why it occurs and what exactly makes it such a painful condition, is not yet clear. But the very vigorous inflammatory reaction caused by the presence of the calcium crystals results in the formation of very excitable nerves and this further exacerbates the pain.
The inflammation not only occurs in the tendon, but also in the bursa that overlies the tendon. The bursa is usually red, swollen and inflamed. In chronic calcific tendinitis, the inflammation is usually much less vigorous.
We are not sure why some patients get acute calcific tendinitis while some may have the calcium deposit for a long time and finally present with chronic calcific tendinitis.
Will the calcium deposit ever go away?
Yes, the calcium deposit in acute calcific tendinitis often does resolve with time. This may occur as quickly as within 1 – 3 months. I have found that chronic calcific tendinitis tend not to resolve spontaneously.
How can calcific tendinitis be treated?
Because acute and chronic calcific tendinitis behave so differently, it is easier to discuss their treatment separately.
Treatment of Acute Calcific Tendinitis
Medications
The first line of treatment is pain relief. A course of anti-inflammatory medications is usually given. This will usually help to dull the pain. Other pain medications can also be prescribed in addition to the anti-inflammatory medications.
In many cases, the pain does start to recede in a week or two. While this may be a preferred option for some patients, others may be in too much pain to tolerate.
Ultrasound guided needle barbotage
This procedure involves locating the calcium deposit using an ultrasound scan, using a needle to physically break up the calcium deposit and usually giving a dose of steroids in the area to reduce the inflammation.
Relief from the pain takes about a week or two. The problem with this procedure is that it is often very painful for the patient. In addition, due to the viscous nature of the calcium deposit, it is not easy to suck it up, even with a large bore needle.
In addition, a lot of calcium is liberated into the bursa which often transiently worsens the inflammation. The thought of having to endure a painful procedure, followed by the prospect of having even more pain for a few days after the procedure is often unthinkable for a patient who is already in distress from the pain.
Arthroscopic evacuation of the calcium deposit
This is a keyhole surgery which is performed under anaesthesia. Under direct vision, the calcium deposit is located, liberated and removed. Most, if not all, of the calcium deposit can be removed.
In addition, the inflamed and occasionally fibrous bursa is removed. I usually finish off with a small dose of steroids which helps to further suppress any remaining inflamed tissue. The pain relief from this procedure is usually dramatic.
This arthroscopic procedure has the added benefit of allowing me to repair any defects in the tendon left after the calcium deposit has been removed. Please refer to the page on Keyhole Surgery to learn more.
Treatment of Chronic Calcific Tendinitis
Medications
Anti-inflammatory medications are useful to dull the pain, but are not the answer in the long term. I often prescribe anti-inflammatory medications as an adjunct to other non-invasive treatment like physiotherapy.
Physiotherapy
Physiotherapy, together with other treatments directed at pain, are useful for pain control. Although physiotherapy is not likely to help resolve a chronic calcific deposit, it may help to improve the pain but improving the way the patient moves the shoulder.
Shockwave Therapy
Some physiotherapists and sports physicians may use shockwave therapy to disrupt the calcium deposit in order to encourage the body to absorb the calcium deposit. The drawback of this is that it is often painful and may aggravate the inflammation due to irritation and disruption of the deposit.
Steroid injections
Steroid injections delivered into the subacromial bursa can help to reduce the pain from the presence of the calcific deposit. It, alone, is not likely to make the deposit disappear. The pain often may also recur after a few months.
Arthroscopic evacuation of the calcific deposit.
For stubborn chronic calcific tendinitis, removal of the deposit surgically is a very reliable and gratifying procedure. Not only can the calcium deposit be removed, defects left in the tendon by the presence of the calcium deposit can also be repaired at the same sitting.
What should I do now?
If you have managed to get to this part of this long article, your shoulder must be bothering you significantly! Consult your family doctor or see an orthopaedic specialist and he/she should be able to advise you accordingly.
 Dr Bryan Tan
Dr Bryan Tan